

ACDF vs. Cervical Disc Replacement: Which Is Right for You?
By Derek G. Ju, MD — Board-Certified Spine Surgeon serving Long Island, Nassau County, and Greater NYC
If you've been told you need neck surgery, you may have more options than you realize. Two of the most common procedures for treating herniated discs and nerve compression in the neck are anterior cervical discectomy and fusion (ACDF) and cervical disc replacement (CDR), also called cervical arthroplasty. While both procedures generally address the same underlying problem, they work differently.
As a minimally invasive spine surgeon in Great Neck and Huntington, Long Island, I perform both procedures and tailor the approach to each patient's anatomy, age, activity level, and goals. Here's an honest breakdown of the differences, so you can have a more informed understanding prior to considering surgery.
What is ACDF?
Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed spine surgeries in the United States, and one of the most successful and reliable surgeries with generally great outcomes. "Anterior" means the surgery is performed through the front of the neck, which gives the surgeon direct access to the disc without disturbing the major muscles of the back of the neck.
During ACDF, the damaged disc is removed, any bone spurs or disc herniations compressing the nerve or spinal cord are addressed, and then a metal spacer is placed to replace the empty disc space, sometimes with a small titanium plate to hold the bones together. Over the following months, your bone grows into the artificial spacer to connect the vertebral bodies into a single, solid segment.
ACDF is typically recommended for:
- Herniated cervical discs causing arm pain, numbness, or weakness
- Cervical radiculopathy (pinched nerve in the neck)
- Cervical myelopathy (spinal cord compression causing spinal cord dysfunction)
- Cervical stenosis (spinal cord or nerve compression)
- Degenerative disc disease with instability
- Cervical kyphosis (poor posture causing the neck to bend forward)
- Patients who are not candidates for disc replacement
What recovery looks like:
Most patients go home the same day or after one night in the hospital. A cervical collar is generally worn for a few weeks to protect the neck. Light activity resumes within 1–2 weeks for most patients, with full recovery and fusion typically occurring over 3–6 months.
ACDF has an excellent long-term track record — decades of outcomes data support its effectiveness for the right patients. It is powerful to remove compression on the nerves and spinal cord, reconstruct and re-align the bones in the neck, and increase the space between the bones to improve posture. I always say that the surgery makes the patient slightly taller and that’s true, by restoring space and alignment between the bones. The trade-off is that fusion eliminates motion at that segment of the spine permanently.
What is cervical disc replacement?
Cervical disc replacement (CDR) — also called cervical arthroplasty — takes a different approach. Instead of fusing the vertebrae together after removing the damaged disc, an artificial disc device is implanted in the empty disc space. This artificial disc allows the vertebrae to continue moving, twisting, and bending — preserving the natural motion of the cervical spine.
Think of it like a hip or knee replacement: rather than fusing the joint, you replace the damaged component while keeping the joint functional.
At my practice, I use several artificial disc devices depending on each patient's anatomy and the specific levels involved, including the Prodisc C, Mobi-C, and Simplify disc systems. Each has specific design characteristics that make it better suited to different patient profiles — another reason a personalized evaluation matters.
Cervical disc replacement is typically recommended for:
- Herniated cervical discs causing radiculopathy (arm pain, numbness, or weakness)
- Degenerative disc disease at one or two levels
- Younger, more active patients who want to preserve motion
- Patients concerned about adjacent segment disease (see below)
- Those who are appropriate surgical candidates based on anatomy and bone quality
What recovery looks like:
Recovery from cervical disc replacement is often faster than ACDF because there's no fusion to wait for. Many patients return to light activity within 1–2 weeks and resume more demanding activity sooner than fusion patients. There's no need to wait for bone to grow — the implant functions immediately.
The adjacent segment disease question
One of the most important reasons patients and surgeons consider disc replacement over fusion is the concern about adjacent segment disease. When a segment of the spine is fused, the segments above and below it take on additional stress to compensate for the lost motion. Over time — typically years to decades — this extra load can accelerate degeneration at those neighboring levels.
Cervical disc replacement, by preserving motion at the treated level, distributes forces more naturally and may reduce the risk of adjacent segment problems down the line. For younger, active patients who have many decades ahead of them, this is a meaningful consideration.
That said, long-term data on disc replacement is still maturing compared to the decades of outcomes data available for ACDF. Both procedures have strong track records — the right choice depends on the individual patient.
Who is — and isn't — a candidate for disc replacement?
Cervical disc replacement sounds appealing to many patients, and for the right candidate it's an excellent procedure. But not everyone qualifies. Factors that may make you a better candidate for ACDF than disc replacement include:
- Significant arthritis or bone spurs at the affected level — disc replacement works best when the joints in the back of the spine are in reasonable condition. Disc replacements don’t address or replace the joints in the back of the spine, only the disc in the front. ACDF is stronger to restore height and alignment of the disc space if the current disc space is collapsed (“bone on bone”).
- Osteoporosis — bone quality affects how well an implant integrates, disc replacements are not recommended in patients with osteoporosis
- Cervical myelopathy (spinal cord compression) — fusion is often preferred for cord compression cases to ensure no further motion at the area that can cause further injury or irritation to the spinal cord
- More than two levels requiring treatment — disc replacements are currently only FDA approved for up to 2 levels
- Prior cervical surgery at the same level
- Certain anatomical variations that affect implant sizing and fit
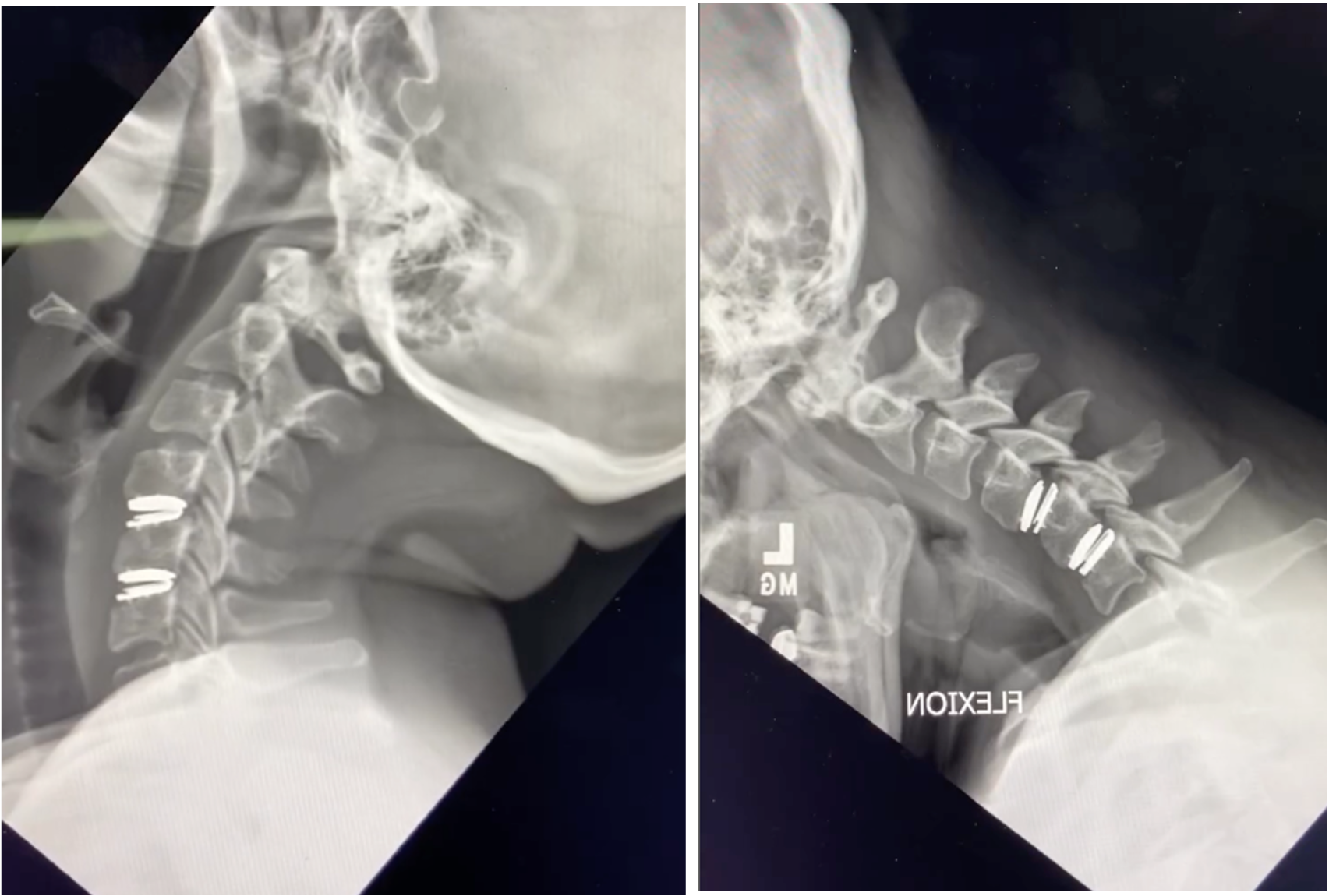
This is why a thorough evaluation — including a review of your MRI, dynamic X-rays (including flexion/extension XR), and full clinical picture — is essential before deciding between these two procedures. A surgeon who recommends one approach without carefully considering the other may not be offering you the full picture.
Dr. Ju's approach: matching the procedure to the patient
I perform both ACDF and cervical disc replacement. My job is to figure out which procedure gives each specific patient the best long-term outcome.
When a patient comes to me with neck and arm pain, I review their imaging personally, assess their symptoms, consider their age and activity level, and then have an honest conversation about which approach makes the most sense — and why. If you're a candidate for disc replacement and would benefit from motion preservation, I'll tell you. If ACDF is the more appropriate choice given your anatomy or the nature of your compression, I'll explain that too.
What I won't do is push one procedure because it's faster or simpler. The goal is always the same: getting you back to your life with the best possible long-term result.
What if I need surgery at more than one level?

Multi-level cervical disease is common, and it's one of the more nuanced decisions in spine surgery. When two or more disc levels need to be addressed, there are three general approaches:
Fusion at all levels (multi-level ACDF) The most established approach for multi-level disease. Each affected disc is removed and the segments are fused together. This is highly effective and has decades of outcomes data and is better at restoring posture and disc height.
Disc replacement at all levels (multi-level arthroplasty) For carefully selected patients, disc replacement can be performed at two levels simultaneously — preserving motion at both. Multiple devices are FDA-approved for two-level cervical disc replacement. Outcomes data for two-level arthroplasty is strong and growing. This is typically best suited to younger, active patients with good bone quality and minimal arthritis at both levels. There are no devices FDA approved for 3 levels or more.
Cervical hybrid surgery — a fusion at one level, disc replacement at another This is where personalized decision-making becomes most important. A hybrid procedure combines ACDF at one level with disc replacement at an adjacent level. The goal is to address each level with the approach that's most appropriate for its specific condition — preserving motion where the anatomy supports it, and fusing where stability or bone quality demands it.
For example: if a patient has a herniated disc at C5-6 that is a good candidate for disc replacement, but significant arthritis and bone spurs at C6-7 that make fusion more appropriate, a hybrid procedure treats both levels optimally rather than applying a one-size approach to the whole spine.
Hybrid surgery requires a surgeon experienced in both techniques. The right multi-level strategy depends on your specific anatomy, the nature of the compression at each level, your age and activity demands, and your bone quality. It's one of the more individualized decisions in elective spine surgery, and it's exactly the kind of conversation I have with every multi-level patient before recommending a plan.
Frequently asked questions
Is cervical disc replacement covered by insurance?
Yes — cervical disc replacement is FDA-approved and covered by most major insurance plans for appropriate candidates, including Medicare. Coverage depends on meeting specific clinical criteria, which I review with each patient during consultation. Hybrid surgery is not covered by all insurance plans, however.
How do I know which procedure I need?
You'll need a thorough evaluation including an MRI of your cervical spine and dynamic XR of your cervical spine (pictures of your neck in different positions). Bring any existing imaging to your consultation — I review every scan personally and will walk you through exactly what I see and why I'm recommending a particular approach.
Can I get a second opinion if I've already been told I need ACDF?
Absolutely, and I encourage it. Second opinions before spine surgery are always appropriate. It's worth knowing whether you're also a candidate for disc replacement, and whether your surgeon performs both procedures or primarily one.
What if I need surgery at more than one level?
Multi-level cases can involve a combination of approaches — for example, disc replacement at one level and fusion at another (called a "cervical hybrid" procedure). Each situation is different and warrants an individualized plan.
Ready to find out which option is right for you?
If you've been diagnosed with a herniated disc, cervical radiculopathy, or degenerative disc disease in your neck, or if you've been recommended for ACDF or disc replacement and want to understand all your options, give me a call.
Dr. Derek Ju, MD offers same or next day consultations at two Long Island locations:
- Great Neck: 600 Northern Blvd, Suite 300, Great Neck, NY 11021
- Huntington: 532 New York Ave, Huntington, NY 11743
Call: (516) 627-8717
Book online:Request an appointment or Book on Zocdoc
In-network with Aetna, Empire BCBS, Cigna, UnitedHealthcare, Oxford, Medicare, Workers Compensation, No-Fault, and most major insurance plans.
Derek G. Ju, MD is a board-certified, fellowship-trained orthopedic spine surgeon specializing in minimally invasive and complex spine surgery. He trained at MIT, Johns Hopkins School of Medicine, Cedars-Sinai Medical Center, and the Rothman Orthopaedic Institute. He is an adjunct associate professor of orthopaedic surgery at NYU Langone Health and has served as team physician for the Philadelphia Eagles, Philadelphia Phillies, Philadelphia 76ers, Los Angeles Rams, and Los Angeles Clippers.
Related reading:
- When is spine surgery actually necessary? A surgeon's honest guide
- Get a second opinion on spine surgery on Long Island